
Case Study 3
- Matron

- Dec 13, 2024
- 5 min read
Asthma or COPD in a 59 year old woman?
A 59 year old woman presents with a cough and wheeze. She is a current smoker.
While it is tempting to assume that this is going to be a case of COPD, it is important that you don't jump to that conclusion until you have all the facts and the before-and-after bronchodilator spirometry test results.
While it is true that 90% of COPD is caused by cigarette smoking, did you know that only around 50% of all smokers go on to develop clinically significant COPD?
I've lost track of how many patients have been incorrectly diagnosed with COPD just because they had a respiratory symptom and a history of smoking.
Back to our case study...
Initial spirometry test result is as follows:

The first thing to look at is the lower limit of normal (LLN) for the FEV/FVC ratio, which here is 0.67. If the actual FEV/FVC ratio falls below the LLN, it would suggest airway obstruction. However, as observed, the actual LLN is 0.69, which exceeds the LLN, indicating no airway obstruction.
Next, turn your attention to the FEV1 which at 1.76 is less than the LLN of 1.77 and only 75% of the predicted. This suggests that something isn't quite right here. A reduced FEV1 in the presence of a 'normal' FEV/FVC ratio can sometimes be suggestive of the presence of a restrictive defect but if you look at the FVC you can see that this is greater than the LLN FVC and greater than 80%.
Now, at this point, you might well be losing the will to live and wishing you had chosen to be the practice diabetic nurse, but before you start wondering if you will ever get your head around spirometry, just remember that you are only halfway through the assessment. Before you can start to make any sense of the initial data, you need to find out what happens to the patient's lung function data after you have given them a bronchodilator!
THINK DIABETES!
Back in the olden days, we diagnosed diabetes by using a Glucose Tolerance Test (GTT). The patient was asked to fast overnight, then they would turn up at the surgery, and we would take a fasting blood glucose level. After that, we would give them a drink that contained 75g of pure glucose. We then took a second blood glucose test 2 hours later, and we would compare the pre- and post-glucose test results. From this, we were able to assess for diabetes or impaired glucose tolerance. It wasn't uncommon for patients to have a perfectly normal fasting glucose and a raised 2-hour glucose level indicating the presence of impaired glucose tolerance. What we didn't do was to interpret the fasting blood glucose test in isolation and ignore the 2 hour glucose test result just because the fasting was 'normal'. A GTT enabled us to assess how the patient responded to a bolus of pure glucose and from that response we were able to formulate a diagnosis.
The pre- and post-bronchodilator test employed in respiratory diagnostics is similar in approach, except that it evaluates the patient's response to a 'bolus' of bronchodilator. Just as a GTT should not be interpreted solely on the fasting blood glucose level, a spirometry test result should not be judged based only on the pre-bronchodilator result. It is essential to compare the results before and after to gain a clearer understanding of the situation.
Back to our case study...
We knew that it was unlikely that the patient had clinically significant COPD after the initial test result as her ratio was greater than her LLN but what it couldn't tell us was whether or not she had asthma!
Asthma and COPD are both chronic obstructive diseases affecting the airways. However, the key distinction is that in asthma, the obstruction is reversible, whereas in COPD, the obstruction is permanent.

However, be aware that if chronic asthma is not treated, it can become irreversible in about 20% of patients. Distinguishing it from COPD relies more on clinical history and other test results like FeNO.
Our case study post SABA spirometry test result is as follows:
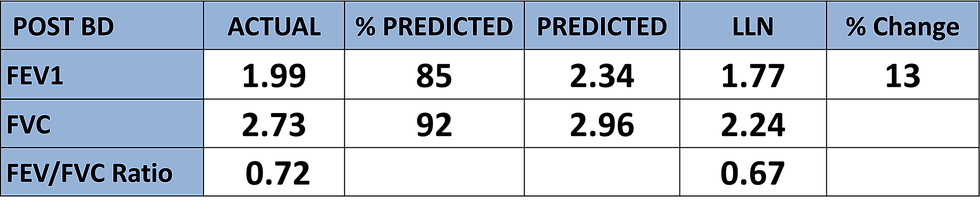
With reversibility testing we are focusing on how the airways respond to a 'bolus' 400mcg dose of a short acting beta agonist (SABA). As it takes around 15-20 minutes for the SABA to work we need to wait this long before we repeat the spirometry test. What we are interested in is how much the FEV1 increases in response to the SABA. NICE guidelines state that a positive test result is recorded when the FEV1 increases by 200ml and 12% or more.
So lets see how our patient has done...
Her FEV1 has gone up from 1.76 litres to 1.99 litres
For ease of maths, convert the litres into millilitres > 1990 - 1760 = 230
Here we see that the FEV1 has increased by 230ml and 13% which meets NICE guideline criteria for a positive test result indicating that our patient does indeed have asthma
What about COPD? Surely she must have some COPD? I hear you all shouting!
To help answer this question I am going to use another diabetes analogy!
As you all know, I am as old as Methuselah and started practicing nursing around the same time that Florence Nightingale was still in clinical practice. Well, way back then we had never heard of pre-diabetes; a patient either had it or not, there was no pre-this or that or impaired fasting glucose or glucose intolerance. Patients were often diagnosed with diabetes after they had a heart attack or stroke. We just didn't do disease prevention or health promotion; we waited for the vascular event and then got involved.
It was eventually found that individuals experience a phase of glucose intolerance before progressing to full-blown diabetes. It was suggested that by identifying people at this stage, we might prevent the progression to full-blown diabetes, leading to the creation of the pre-diabetes register.
Well, that's where we are going with COPD!
The latest set of GOLD Guidelines are calling for the recognition of a state of pre-COPD and state the following:
Some individuals exhibit respiratory symptoms or structural lung abnormalities, such as emphysema, gas trapping, hyperinflation, or reduced lung diffusing capacity, without meeting the diagnostic criteria for airflow obstruction (post-bronchodilator FEV₁/FVC ≥ LLN). These individuals are categorized as "Pre-COPD." Additionally, the term "PRISm" (Preserved Ratio Impaired Spirometry) is used to describe those with a normal FEV₁/FVC ratio but abnormal spirometric findings. Both Pre-COPD and PRISm individuals are at risk of developing airflow obstruction over time, although this progression does not occur in all cases.
Our case study presented with a preserved FEV1/FVC ratio and abnormal spirometric findings (reduced FEV1), so could well have met the criteria for pre-COPD had she NOT had a positive response to SABA reversibility testing.
Ultimately, the fact that our patient does not have COPD at present does not rule out the possibility of her developing it (alongside her asthma) in the future. We understand that individuals with asthma who smoke have a heightened risk of developing COPD. However, it's crucial to note that when this occurs, COPD does not replace asthma. At that stage, the patient will have two distinct airway diseases.
I hope you have found this case study useful.


Comments